A 64 year old man with altered sensorium who is unable to speak
- This is an a online e log book to discuss our patient's de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centred online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment.
Date of admission: 28.12.22
A 64 year old male came to OPD with Chief complaints of
Unable to speak since 8 days

HOPI : The patient was apparently asymptomatic 13 days back then he developed cough which is insidious in onset and gradually progressive in nature. It is productive type which subsided on using medication.
He developed bowel and bladder incontinence along with loss of appetite since 13days.
He developed hiccups and loose stools 10 days back about 5 episodes per day last for 1 day where he was taken to a local doctor which subsided on taking medication.
And then since 7 days he stopped speaking and then was brought to our hospital
Past history:
He is a known case of type 2 DM since 7years and is taking medication metformin and glimiperide since 4yrs.
No h/o HTN, asthma, epilepsy,CAD
Personal history :
He used to work as a cattle rearer. Since the time he was diagnosed with diabetes he worked infrequently. From past 3 years he has stopped working as he is unable to walk without using stick. There is also drastic loss of weight since he became diabetic.
Appetite - Lost
Diet - Mixed
Bowel and bladder movements - incontinence
(from past 2 days - constipation)
Addictions - Occasional alcoholic ( during functions ) tobacco chewing daily since last 30 yrs
No food / drug allergies
Family history:
His daughter had TB 7 yrs back and was treated
His mother had TB 5 yrs back and was treated
General examination :
Patient is conscious, incoherent and uncooperative
He is moderately built and nourished
Pallor : present
Icterus : absent
Cyanosis: absent
Clubbing : absent
Lymphadenopathy : absent
Edema : absent


Vitals :


Temp : 97.3 f
Pulse : 100bpm
RR:20cpm
Bp:110/60
Spo2: 98%
Grbs: 193 mg/dl
Systemic examination -
CNS -
GCS :
E4,V1,M1
Sensory system -
Pain , touch(fine & crude) , temp, vibration, joint position - no response
Motor system -
Right Left
Tone - UL Hypo Hypo
LL Hypo Hypo
Power - UL and LL no movement even with pain
Reflexes - not elicited
Brain stem reflexes -
B/L corneal + , conjunctival + , pupillary +
Cranial nerves - intact
Finger nose in coordination - no
Heel knee in coordination - no
CVS - S1,S2 heard, no murmurs ,no thrills
Respiratory system - decreased air entry on left side, crackles are heard, position of trachea - central
Abdomen - soft, non tender , no organomegaly

















usg

Provisional diagnosis:
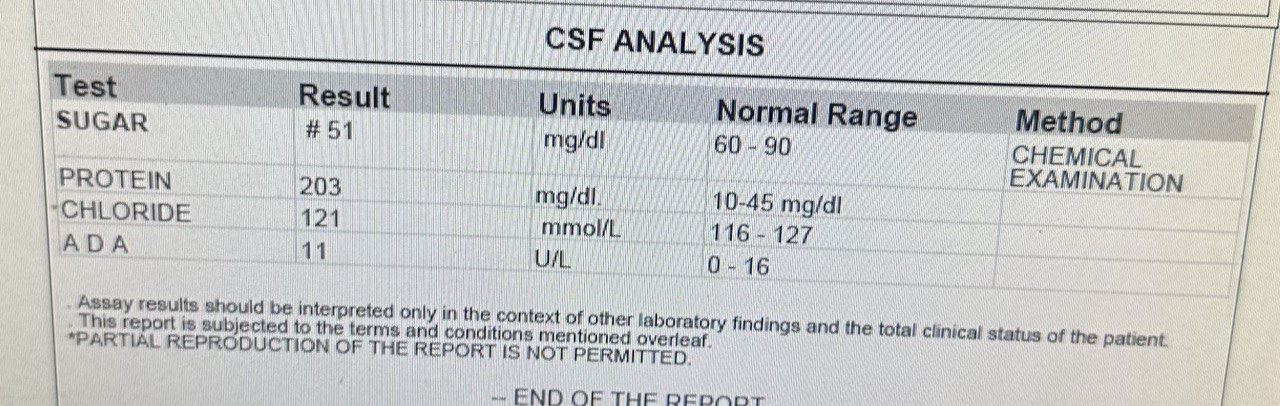
Altered Sensory secondary to meningoencephalitis,
Left sided pneumonia (Tb?)
Bilateral flex ion deformity since 2 years
Treatment plan:
03/01/2023
1) IVF 0.9 %NS IV @ 100 ml / hr
2) Nebulization with duolin - 8th hrly , budecort - 12 th hrly
3) Inj .Thiamine 200 mg IV/BD in 100 ml NS
4) Inj . Dexa 6 mg IV / TID
5) ATT therapy PO/OD FDC:3 tab/ day
6) GRBS monitoring 6 th hrly
7) vitals monitoring 6 th hrly
8) Temp monitoring 4 th hrly
9) Inj H. Actrapid insulin SC TID acc to GRBS
10)RT Feeds - 100 ml milk +3-4 scoops protein powder 4 th hrly , 50 ml H2O 2nd hrly
11 ) physiotherapy was done
04/01/2023
1) IVF 0.9%NS IV@ 100ml/hr
2) inj.Thiamine 200mg IV/BD in 100ml NS
3) inj Dexa 8mg iv/TID
4)ATT therapy PO/OD 3tab/ day
5) monocef 2gm iv BD
6)TAB ivabrad 5mg
7)perinorm 20mg


Comments
Post a Comment